Musculoskeletal injury and the correlation with foot plantar pressure in an Australian Aboriginal population
Brief reportCharles J (2018)
Musculoskeletal injury and the correlation with foot plantar pressure in an Australian Aboriginal population. Australian Indigenous HealthBulletin 18(1). Retrieved [access date] https://healthbulletin.org.au/articles/musculoskeletal-injury-and-the-correlation-with-foot-plantar-pressure-in-an-australian-aboriginal-population
Corresponding author: Associate Professor James Charles, The Institute of Koorie Education and the School of Medicine
Deakin University, Waurn Ponds Campus
Lock Bag 20000, Geelong Victoria 3220, Australia
Ph: +61 35227 8694, mobile +61422674295, Email: james.charles@deakin.edu.au
Abstract
Objectives: There has been limited research into Aboriginal foot biomechanics and musculoskeletal injury. Studies have shown Aboriginal people have high rates of back injury, but no explanation of the cause has been provided or investigated. This study will examine the prevalence of ankle, knee and back injury and the association with foot pressure.
Methods: A total of 127 Aboriginal community members volunteered for a clinical assessment of foot pressure and musculoskeletal injury. Analysis of plantar pressure was recorded in both the left and right feet. The Tekscan HR Mat system was used to investigate Peak Pressure (PP) and Pressure Time Integrals (PTI). Participants were asked to self-report if they previously or currently have an ankle, knee or back injury.
Results: There were 80 (67%) participants who self-reported that they had a previous ankle injury and 36 (30%) had a current ankle injury. There were 61 (52%) who reported having a previous knee injury and 32 (27%) who had a current knee injury. There were 75 (64%) who indicated they had a previous back injury, and 53 (45%) who had a current back injury. Musculoskeletal injury was high, with knee injury being associated with mid-foot pressure, mid-foot PP left -.276**, mid-foot PTI left -.362**, and mid-foot PTI right -.321** and back injury with mid-foot PTI right -.259**.
Conclusions: Aboriginal people have concerning percentages of musculoskeletal injuries which are correlated with mid-foot pressure. Ankle, knee and back injuries can be debilitating, which may have a direct effect on health but also impact on participation in sport, and other physical activities, including cultural activities.
Implication: The correlation of mid-foot pressure and musculoskeletal injuries may impair some Aboriginal community members’ ability to participant in physical and cultural activities, which may also effect quality of life and social and emotional well-being of community members.
Key words: Aboriginal, Barefoot, Plantar-Pressure, and Injury
Acknowledgement: I would like to acknowledge and thank the Awabakal, Worimi, Biripi, Darug Aboriginal communities for their participation and support of this research.
Disclaimer: In some instances in this paper I will be using the term ‘Aboriginal’ to describe both Aboriginal and Torres Strait Islander peoples. This is due to word restrictions and brevity, and no disrespect is intended to any individual or group.
View PDF version (719KB)
Introduction
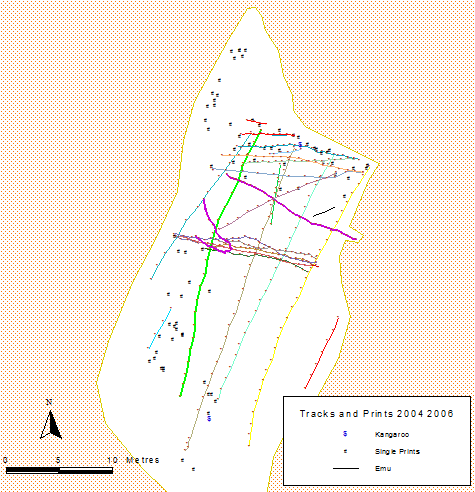
Aboriginal Australians are athletic, and they have been for many thousands of years [1,2], this has been an evolutionary process [3], developed through survival skills required to thrive in a very harsh environment [4]. Sport and physical activities are also very important to many Aboriginal cultures, not just for survival but culture, with ball games being played by many different tribes [2,5]. Being athletic was also required for hunting, and this would have required great physical fitness and athleticism [6]. The great running speed of ancient Aboriginal Australians has been documented in foot prints at Lake Mungo in the Willandra Lakes area of NSW [7,8]. All the footprints at Lake Mungo have been GPS marked (Figure 1), some of the men running, are taking approx. 25 steps to travel an approx. 50 metres (Figure 1) or 50 steps to travel 100 m. This stride pattern is similar to some of the modern world’s fastest athletes. Usain Bolt took 41 steps to travel 100 metres to win the gold medal in the London 2012 Olympic games, to reach a top speed of 37 km/h [9]. Using 50 steps to travel 100m would take an estimated 10 seconds to run 100 m [10]. Using a pace calculator [11] this is an estimated top speed of 35Km/h. It must also be considered that these men were running barefoot, in the mud, and likely carrying a weapon(s) and/or other item(s). It must be considered that these calculations of the ancient Aboriginal men running 100 m is an estimate based on an extrapolation of a 50m run, and there is no way of knowing if these men could have maintained this stride pattern. This athleticism of Aboriginal people has continued with modern Aboriginal men participation in the Australian Football League (AFL) and Nation Rugby League (NRL) [12]. With the importance of participation in sport at all levels for not only individuals regularly playing sport but also the general Aboriginal population wanting to participate in physical cultural activities, injury diagnosis, and better practices to limit injuries is extremely important to investigate.
Figure 1: GPS Tracking of Footprints, yellow, green and grey and trackways of Aboriginal men running (Image courtesy of the Willandra Lakes Region World Heritage Area Technical and Scientific Advisory Committee and the Community Management Council).
There has been limited research into musculoskeletal injury in the Australian Aboriginal community, and the research available has only concentrated on back injury, with one study showing the most common musculoskeletal injury in rural and remote areas was lower back injury [13]. Research has shown a higher prevalence of chronic musculoskeletal problems in an Aboriginal population than in a non-Aboriginal population [14]. A study of chronic conditions in an urban Aboriginal population found that 14% of chronic conditions were musculoskeletal problems [15]. Previous research also reported that approximately 30% of Aboriginal men and 50% of Aboriginal women had a long term lower back complaint [16] and similar injuries were reported in Indigenous communities internationally [17]. Many of these studies reported on older Aboriginal people but a report investigating young (18-38 year old) Aboriginal rugby league players (n=24), found 46% had a back injury in the past 2 years [18] however these injuries may have been a result of participation in contact sport. The prevalence of musculoskeletal injuries has been found to be higher in Aboriginal Australians compared to non-Aboriginal Australians and the burden is greater for Aboriginal people [19]. Aboriginal Australians are also only half as likely to receive professional health care service than other Australians or receive a knee or hip replacement if needed [19]. This study is designed to investigate the level of musculoskeletal injuries in an adult Aboriginal population in a non-specific cohort and investigate foot pressure that may provide more information about these injuries. No previous study has investigated why musculoskeletal injury is so high in Aboriginal peoples, however it was proposed perhaps labouring type of employment may be related [13] but this hypothesis was not investigated. It has been hypothesized by the author of this study that the high prevalence of musculoskeletal injuries may be due to mid-foot peak pressure (PP) and or mid-foot pressure time integrals (PTI) seen clinically. This study was designed to investigate if there is any correlation between either mid-foot PP and or PTI with knee and or back injury.
Ethics Approval
Ethical approval was granted from the Human Research Ethics Committee (HREC) at the University of Newcastle (Protocol Number 2012-0385) and the Aboriginal Health and Medical Research Council Ethics Committee (Reference Number 895/12). Three Aboriginal communities participated in this study, Mt Druitt (Western Sydney), Newcastle (Hunter Region) and Forster (Mid North Coast) in New South Wales, Australia. Four Aboriginal organizations supported this project, Western Sydney Aboriginal Medical Service (Mt Druitt), Awabakal Aboriginal Medical Service (Newcastle), the Wollotuka Institute (Newcastle), and Tobwabba Aboriginal Medical Service (Forster), NSW, Australia.
Methods
The participants that agreed to take part in the study were assigned an identification number to de-identify results. All participants were required to be an Aboriginal person, over 18 years old, and be able to stand and walk independently. After volunteering and signing a consent form, nine participants were unable to attend to complete the assessment and decided to withdraw from the project.
There are many foot pressure analysis devices on the market and they are used regularly for clinical biomechanical assessments and research. [20-22] The Tekscan Pressure Measurement System, Copyright TekScan Inc. 1998-2013 was chosen as the most appropriate device, because of its mobility, light weight, small size, and ease of use. [23]
The reliability of TekScan device for barefoot pressure analysis for children (7-11 years) was reported as ‘moderate to good’ (0.69-0.93) at different points of the foot, with the exception of the lesser toes which showed poor reliability [24]. A reliability study of TekScan MatScan conducted on adults (over 18 years), also showed ‘moderate to good’ reliability with intra-class correlation ranging from 0.44 to 0.95 for the mean across seven different areas of the foot, but again finding that the lesser toes was the least reliable [25]. Research by Gurney et al 2008, found general good reliability for TekScan but reliability was higher for high loading areas such as the forefoot [26]. In this project the TekScan device was used to analyse barefoot pressure on five areas of the foot (Figure 2) i.e. the hallux, 1st metatarsophalangeal joint, 2nd-5th metatarsophalangeal joint, mid-foot and heel of both left and right feet (Figure 2). The lesser toes were not analysed due to poor reliability reported in previous studies [24,25].
Figure 2: Five sections of the measured barefoot pressure
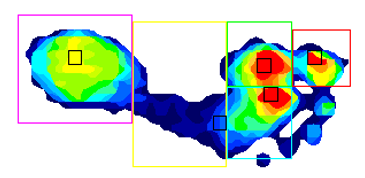
Note: Colour coding is for each section measured
The TekScan mat is light weight, 5mm thick, 432mm by 368mm rectangle, with 2288 sensors, which participants were required to walk over. There are three different procedures with TekScan to measure foot pressure i.e. 1-step, 2-step and 3-step protocol, prior to stepping on the mat, these where examined as to which would be most appropriate for this study [27]. A comparative study of the 1-step, 2-step and 3-step protocols showed Peak Pressures (PP) and Pressure-Time Integrals (PTI) were not significantly different between the three protocols [27]. Although contact time was significantly different for the heel between 1-step and 3-step methods (P<0.05), and the 1-step and 2-step protocols were most reliable but the 2-step required less repeated trials and was recommended as the most appropriate [27]. The two step protocol was also found to be as reliable as the mid-gait method, and more reliable in most foot areas [28]. Due to the recommendation of previous studies [27,28], and the requirements of this study, a two-step protocol was incorporated.
Participants were asked to remove their shoes and socks, then weighed, which is required for calibration of the TekScan device, as per the developer’s instructions. Once calibration was complete, the 2-step protocol was explained and demonstrated to participants. Three recordings were taken of each foot, for each participant, and the mean was calculated, as this was found to be an appropriate number of readings to produce reliable pressure data [29]. Recordings were repeated if for any reason participants altered normal gait or strayed off the mat.
Injury questionnaire
The Aboriginal Multiple Injury Questionnaire (AMIQ) was used to assess participants musculoskeletal injury [30] for this study. The AMIQ is culturally appropriate, client centred questionnaire which is specific for Aboriginal people, but only asks basic demographic data i.e. residential area, age and gender [30]. The AMIQ asks participants if they have ever had previous and/or have a current ankle, knee and back injury, but the cause of injury is not investigated [30]. These questions are important to establish injury history and current status of injury for participants. The AMIQ assess many aspects of musculoskeletal injury [30], but was only used to assess self-reported ankle, knee and back injury in this study. It is important to note that self-reported injuries for AMIQ may or may not be diagnosed by a health professional [30].
Data analysis
The analysis for barefoot pressure was conducted with F-Scan Research Version 7.00-19 TekScan Pressure Measurement System, investigating Pressure v’s Time, (Figure 3) and Peak Pressure v’s Time (Figure 4) at each of the five foot segments on both left and right foot. The Pressure v’s Time, Pressure Time Integrals (PTI) were recorded in kilopascal/second (KPa*sec) for each foot section indicated by the relevant colour coding (Figures 2 and 3). With Peak Pressure v’s Time, max pressure was recorded for each foot section indicated by the relevant colour coding (Figures 2 and 4). A mean of the three readings was used to determine barefoot pressure of each foot section in both left and right feet.
Figure 3: Pressure vs Time
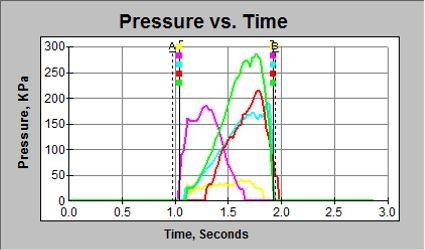
Note: Colour coding for each foot section of the foot from Figure 1
Figure 4: Peak Pressure vs Time
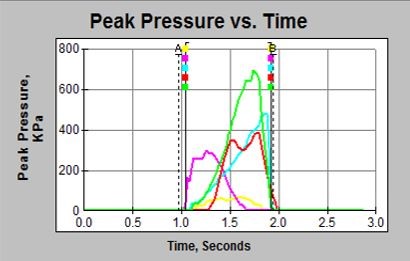
Note: Colour coding for each foot section of the foot from Figure 1
All participants were surveyed about ankle, knee and back injury with AMIQ [30]. Participants were asked if they had ever had an ankle, knee or back injury, and were also asked if they have a current ankle, knee or back injury. Statistical analysis was performed using the Statistical Package Social Science software version 21.0 (SPSS Chicago, Illinois, USA) which was used to calculate percentages of injuries and analyse correlations with barefoot pressure. The correlation were set at * significant at 0.05 level (2 tailed) and correlation ** significant at 0.01 level (2 tailed). Correlation coefficients were interpreted as 0.1 poor/weak, 0.3 moderate and 0.5 strong, as described by Cohen 1988 [31].
Results
A total of 127 Aboriginal community members volunteered to take part in a non-invasive clinical assessment of foot pressure and the AMIQ to assess injuries.
The demographics of participants: 53 (42%) male, 74 (58%) female, age 18-79 years (mean age 51 years). There were 48 (37.8%) who came from Mt Druitt (Western Sydney), 41 (32.3%) came from Newcastle (The Hunter) and 38 (29.9%) came from Forster (Mid-North Coast) NSW, Australia.
When the Aboriginal participants were asked if they had ever had an ankle injury, 80 (67%) stated they had a previous ankle injury and 36 (30%) indicated they had a current ankle injury.
There were 61 (52%) participants who stated they had a previous knee injury and 32 (27%) had a current knee injury and this was found to have a significant correlation at 0.01 level with mid-foot PP left -.276**, mid-foot PTI left -.362**, and mid-foot PTI right -.321**.
There were 75 (64%) of participants indicated they had a previous back injury and this was found to have a significant correlation at 0.01 level with mid-foot PTI right -.259**. When participants were asked if they had a current back injury 53 (45%) indicated ‘yes’, and this was found to have a significant correlation at 0.05 level with mid-foot PTI right -.229*.
Table 1: Foot pressure data (minimum, maximum, mean and SD of combine cohort foot pressure for PP and PTI for each foot section for left and right foot)
| Average of 3 Readings | N | Minimum | Maximum | Mean | Std. Dev |
|---|---|---|---|---|---|
| Heel PP left | 124 | 147.67 | 1032.67 | 372.8495 | 163.6497 |
| Heel PTI left | 124 | 16.33 | 167.33 | 65.636 | 29.34974 |
| Mid-foot PP left | 124 | 25.67 | 618.67 | 181.2258 | 112.3505 |
| Mid-foot PTI left | 124 | 2.33 | 97.67 | 31.6734 | 16.94288 |
| Met 2-5 PP left | 124 | 154.67 | 1362.33 | 495.4086 | 197.2315 |
| Met 2-5 PTI left | 124 | 25 | 138 | 72.2903 | 25.09152 |
| Met 1 PP left | 124 | 85 | 1092.33 | 342.0806 | 200.8044 |
| Met 1 PTI left | 124 | 13.67 | 197.43 | 62.071 | 32.89416 |
| Hallux PP left | 124 | 0 | 1009 | 375.9543 | 212.7867 |
| Hallux PTI left | 124 | 0 | 170 | 54.871 | 35.08553 |
| Heel PP right | 123 | 108 | 1279.67 | 358.0949 | 154.7312 |
| Heel PTI right | 123 | 10.33 | 202 | 59.8407 | 27.97762 |
| Mid-foot PP right | 123 | 60.67 | 2285.67 | 274.6694 | 250.0179 |
| Mid-foot PTI right | 123 | 7.33 | 96.67 | 35.065 | 17.47383 |
| Met 2-5 PP right | 123 | 117.67 | 1075.67 | 490.2195 | 177.9349 |
| Met 2-5 PTI right | 123 | 20.67 | 144 | 77.9751 | 25.87206 |
| Met 1 PP right | 123 | 62.67 | 965.33 | 360.3198 | 197.8387 |
| Met1 PTI right | 123 | 11.8 | 160.33 | 62.8648 | 29.19056 |
| Hallux PP right | 123 | 0 | 977.33 | 374.8997 | 188.6554 |
| Hallux PTI right | 123 | 0 | 180 | 52.2003 | 28.80297 |
Discussion
The percentages of participants that had previous ankle, knee or back injury is a concern, especially for the impact on activity and the ability to participate in sport in the past, present and future. Current injury percentages were also concerning for participants with approx. There were 1 in 3 having reporting a current ankle and knee injuries and half having a back injury. These results indicate that Aboriginal people in these communities experience high occasion of injuries. There has been little investigation in to ankle injury in Aboriginal populations, but a report with a very small sample (n=24) showed 42% had an ankle injury in the past 6 months [18], which is similar to the findings in this study. There has also been little investigation in to knee injury in an Aboriginal population, but a report (n=24) stated 25% of participants had a knee injury in the past 6 months [18], which supports the findings of high percentages of knee injury in this study, indicating that age may not be related to these injuries. There has been some previous investigation finding high levels of back injury or pain in Aboriginal population [13-16]. The Vindigni et al 2004 study reported 42 (48.3%) Aboriginal male (n=87) and 33 (32.4%) Aboriginal females (n=102) reported having a back injury in the previous 7 days [13]. Others also found similar results for back injury or pain [15-18], and the participants in this study reported very similar percentages for back injury as these previous studies. The results in this study found that knee and back injury was associated with mid-foot PP, but predominately PTI i.e. the amount of time spent on the mid-foot during gait. This increased mid-foot PP and PTI may also be exacerbated by hard ground surfaces e.g. concrete, which Aboriginal people would not have traditionally walked on [6-8]. Indicating that Aboriginal people prior to these hard surfaces being introduced may not have suffered such high percentages of these types of injuries. Although the correlations with musculoskeletal injury and mid-foot PP and PTI in this study were moderate i.e. 0.3 as described by Cohen 1988 [31] but they were significant for both PP and PTI, with 4 out of 5 correlations being PTI. These finding indicate that these Aboriginal people are pausing in mid-stance of their gait, prolonging pressure on the mid-foot. Applying pressure on this area for longer periods of time, and this pause in mid-stance of gait is correlated with knee and back injury in these participants. Ankle, knee and back injuries can be debilitating, causing sufferers to reduce activity, training and sport. This can have effects on health directly but can also limit cultural and social activities. Reduced physical and cultural activities can also effects quality of life and social and emotional well-being for Aboriginal people. Reduction of participation in activity, training and sport can also lead to weight gain, and obesity [32]. Being over-weight or obese is a risk factor for a wide variety of chronic disease [33-35] being over-weight or obese is also very high in Aboriginal communities, especially Aboriginal women [32]. Unfortunately becoming over-weight or obese, and the development chronic disease can lead to premature morbidity and mortality [36].
Limitations
The volunteer groups in this study had approximately equal amounts of males and females, and attempts were made to have approximately equal amounts of volunteers from all three participating communities. However participants were volunteers (not a random sample), the numbers were relatively low and there was no control group without injuries for comparison. Therefore the findings of this project are not representative of all Aboriginal peoples and no causal relationship has been established and caution should be used in interpreting the findings of this study. However the author believes the participants are a representative sample of Aboriginal adults in Western Sydney, the Hunter and Mid-North Coast of NSW and the finding do add to the knowledge of musculoskeletal injuries in the Aboriginal communities that participated.
Conclusion
The findings in this study have identified concerning levels of musculoskeletal injuries in the participants of this study, and may offer some explanation for knee and back injury in these communities. These findings may provide some guidance for health professionals incorporating measures that could reduce these injuries e.g. shoe inserts that can off-load the mid-foot, and improve foot function. Therefore reducing PTI and PP and the risk of musculoskeletal injury, and the associated pain. Reducing PTI and PP may also assist to improve activity and reduce weight gain, which can lead to chronic disease. The assessment and off-loading of foot pressure for Aboriginal peoples may lead to greater and prolonged participation in training, sport, and cultural activities. Incorporating better practices suggested, may also contribute to increased quality of life, social and emotional well-being in the Aboriginal community.
References
- Webb S, Cupper ML, Robins R. Pleistocene human footprints from the Willandra Lakes, southeastern Australia. Journal of human evolution. 2006;50(4):405-413.
- Watkins C, Gale MA, Adelaide SIo, School KP. Kaurna Alphabet Book: With an Introduction to the Kaurna Language. Kaurna Plains School; 2006.
- Webb S. Further research of the Willandra Lakes fossil footprint site, southeastern Australia. Journal of human evolution. 2007;52(6):711-715.
- Westaway M. Footprints of the First Australians. Australasian Science (2000). 2010;31(2):14.
- Robert B. The Aboriginies of Victoria. Vol 11878.
- Grubb PL. Persistence Hunting and the Evolution of Human Endurance Running. Graduate Student Journal of Anthropology.33.
- Johnston H. The Willandra Lakes Region World Heritage Area, New South Wales, Australia: Land Use Planning and Management of Aboriginal and Archaeological Heritage. In: Archaeological Dimension of World Heritage. Springer; 2014:39-55.
- Franklin N, Habgood P. Finger Markings and the Willandra Lakes Footprint Site, South-Eastern Australia. Rock Art Research: The Journal of the Australian Rock Art Research Association (AURA). 2009;26(2):199.
- Ingle S. London 2012: Five reasons why Usain Bolt won the Olymipic 100m final. The Guardian. 06/0812, 2012.
- Faccioni A. Complete Sprinting Technique. 2016; http://www.adriansprints.com/2011/03/complete-sprinting-technique-charlie.html. Accessed 05/06/16.
- Net C. Pace Calculator. 2016; http://www.calculator.net/pace-calculator.html?ctype=pace&ctime=00%3A00%3A10&cdistance=100&cdistanceunit=Meters&cpace=00%3A08%3A10&cpaceunit=tpm&printit=0&x=53&y=9. Accessed 05/06/16.
- Indigenous AFL player numbers drop result of ‘equity issue’, says sports physician. In:2014.
- Vindigni D, Griffen D, Perkins J, Da Costa C, Parkinson L. Prevalence of musculoskeletal conditions, associated pain and disability and the barriers to managing these conditions in a rural, Australian Aboriginal community. Rural and Remote Health. 2004;4:230.
- Mayhew C, Vickerman L. Aboriginal and Torres Strait Islander occupational health and safety: a pilot study in Queensland. Australian Aboriginal Studies. 1996(2):61.
- Tan G. Indigenous health. A needs assessment study of the Outer Eastern Metropolitan Region of Melbourne. Detailed Report March. 1998:26.
- Honeyman PT, Jacobs EA. Effects of culture on back pain in Australian aboriginals. Spine. 1996;21(7):841-843.
- Muirden K. The origins, evolution and future of COPCORD. APLAR J Rheumatol. 1997;1:44-48.
- Charles J. An evaluation and comprehensive guide to successful Aboriginal health promotion. Australian Indigenous HealthBulletin. 2016;16(No 1 January – March).
- Lin IB, Bunzli S, Mak DB, et al. The unmet needs of Aboriginal Australians with musculoskeletal pain: A mixed method systematic review. Arthritis Care & Research. 2017:n/a-n/a.
- Chesnin KJ, Selby-Silverstein L, Besser MP. Comparison of an in-shoe pressure measurement device to a force plate: concurrent validity of center of pressure measurements. Gait & Posture. 2000;12(2):128-133.
- Putti AB, Arnold GP, Cochrane LA, Abboud RJ. Normal pressure values and repeatability of the Emed® ST4 system. Gait & Posture. 2008;27(3):501-505.
- Bachus KN, DeMarco AL, Judd KT, Horwitz DS, Brodke DS. Measuring contact area, force, and pressure for bioengineering applications: Using Fuji Film and TekScan systems. Medical Engineering & Physics. 2006;28(5):483-488.
- Brenton-Rule A, Mattock J, Carroll M, et al. Reliability of the TekScan MatScan® system for the measurement of postural stability in older people with rheumatoid arthritis. Journal of Foot and Ankle Research. 2012;5(1):1-7.
- Cousins SD, Morrison SC, Drechsler WI. The reliability of plantar pressure assessment during barefoot level walking in children aged 7-11 years. J Foot Ankle Res. 2012;5(1):8.
- Zammit GV, Menz HB, Munteanu SE. Research Reliability of the TekScan MatScan® system for the measurement of plantar forces and pressures during barefoot level walking in healthy adults. J Foot Ankle Res. 2010;3:11.
- Gurney JK, Kersting UG, Rosenbaum D. Between-day reliability of repeated plantar pressure distribution measurements in a normal population. Gait & Posture. 2008;27(4):706-709.
- Bus SA, Lange Ad. A comparison of the 1-step, 2-step, and 3-step protocols for obtaining barefoot plantar pressure data in the diabetic neuropathic foot. Clinical Biomechanics. 2005;20(9):892-899.
- Bryant A, Singer K, Tinley P. Comparison of the reliability of plantar pressure measurements using the two-step and midgait methods of data collection. foot & ankle international. 1999;20(10):646-650.
- van der Leeden M, Dekker JH, Siemonsma PC, Lek-Westerhof SS, Steultjens MP. Reproducibility of plantar pressure measurements in patients with chronic arthritis: a comparison of one-step, two-step, and three-step protocols and an estimate of the number of measurements required. foot & ankle international. 2004;25(10):739-744.
- Charles J. The Aboriginal Multiple Injury Questionnaire (AMIQ): The development of a musculoskeletal injury questionnaire for an Australian Aboriginal population. Australian Indigenous HealthBulletin. 2017;17(3).
- Cohen J. Statistical Power Analysis for the Behavioral Sciences. 1988.
- Cameron AJ, Welborn TA, Zimmet PZ, Dunstan DW. Overweight and obesity in Australia: The 1999-2000 Australian Diabetes, Obesity and Lifestyle Study (AusDiab). Medical Journal of Australia,. 2003;178(9):427-432.
- Adler AI, Stratton IM, Neil HAW, et al. Association of systolic blood pressure with macrovascular and microvascular complications of type 2 diabetes (UKPDS 36): prospective observational study. BMJ. 2000;321(7258):412-419.
- Faisal A-M, Khaldoon A-R. Diabetic neuropathy, foot ulceration, peripheral vascular disease and potential risk factors among patients with diabetes in Bahrain : A nationwide primary care diabetes clinic-based study. Annnals of Sudi medicine. 2007;27(1).
- Despres J-P, Lemieux I, Bergeron J, et al. Abdominal Obesity and the Metabolic Syndrome: Contribution to Global Cardiometabolic Risk. Arterioscler Thromb Vasc Biol. 2008;28(6):1039-1049.
- Australian Bureau of S. 2004 – 05 National health survey: Summary of results (No. 4364.0).